



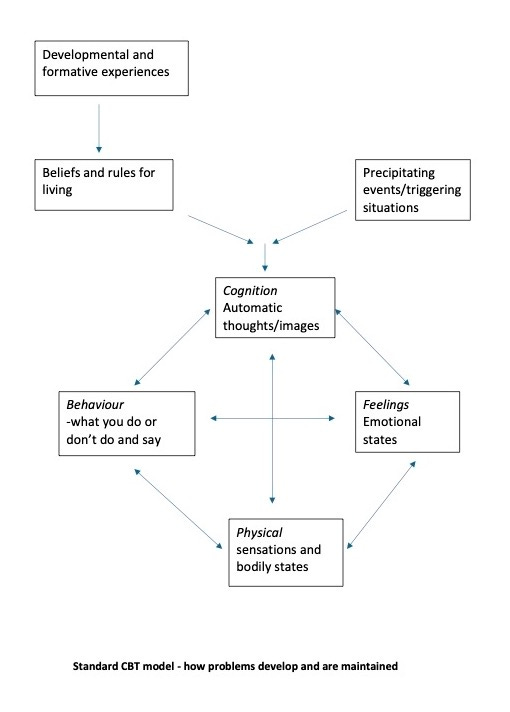
The Standard CBT Model: how your problems develop and why they won't go away
... and why ADHDers need an Enhanced Model -Part 5 of the Fundamentals of CBT

In the previous articles in this series, we’ve explored the individual elements that make up Cognitive Behavioural Therapy (CBT): Thoughts, Feelings, Physical Sensations, and Behaviours. Now, we bring them together into the Standard CBT Model explaining how problems develop and what stops from them going away - the classic framework that underpins traditional CBT interventions.
How the past contributes to the present problem
The CBT model proposes that through key childhood experiences (and some later formative experiences), we develop functional and dysfunctional core beliefs. These beliefs are about ourselves, others and the world.
Functional beliefs are ones that support healthy functioning and interactions; dysfunctional ones hinder our wellbeing and relationships. Dysfunctional beliefs may be distortions, but others may be rigid, overly generalised, or outdated rather than outright false.
We also develop rules for living that guide us into behaving in accordance with this personal worldview. These beliefs and rules allow us to make sense of our world and find our way through it. This is a normal process that occurs in everyone.
If we encounter event/s that trigger a dysfunctional core belief or violate a functional core belief, then unhelpful rules can become rigidly enforced or more dominant, negative thoughts arise and unpleasant emotional states can result, such as anxiety or depression. The problem has been ‘set in motion’.
What keeps the present problems going
The Standard CBT model is often illustrated as a five-part cycle, where each element feeds into the next:
Precipitating events/triggering situation: the external or internal event that sets the cycle in motion.
Cognitions: the thoughts, images and interpretations we have about ourselves, others, and the world.
Feelings (emotions): the emotional reactions triggered by our thoughts and experiences.
Physical sensations (bodily reactions): the physiological responses we experience, such as tension, rapid heartbeat, or nausea.
Behaviours (actions): how we respond, including avoidance, seeking reassurance, or engaging in coping strategies.
Example: anxiety in a social situation
Imagine you were shy as a small child and were made to perform in the school’s Christmas show. You cried on the stage and everyone laughed. Now imagine as an adult, you have to walk alone into a room full of chatting people (triggering situation). Your automatic thought might be, “They’re all judging me and think I’m awkward”. This leads to a feeling of dread. Your body responds with a racing heart and a tight chest. Your behaviour? You might avoid eye contact, stand in a corner, or leave early. Or you might simply not enter the room at all.
That’s an example of a single formative experience shaping a future pattern of social anxiety. But it can also result from repeated exposure to smaller triggers: a mother who frequent admonishes her children to “don’t slouch, people will think you’ve something to hide!“ or getting picked on by other kids for being short or tall etc.
The double headed arrows in the CBT model help us see how these patterns reinforce themselves. The more you think “they’re going to laugh at me”, the more nervous you become, and the more you use escape behaviours. This urge to run away creates yet more mental imagery of other similar public appearances and the more you sweat and tremble. And so on. You’re locked in a vicious cycle, where your problem has been ‘switched on’ and is being maintained by these interactions. This vicious cycle prevents the problem from being ‘stopped’, even once the circumstances change.
If your behaviour is always therefore to avoid social situations, you never gather evidence to challenge your negative thoughts about being judged, and the cycle continues. Of course, maybe no one in the room was thinking about you at all, but you’ll never know because you never test that belief against reality.
Breaking the cycle: why CBT focuses on thoughts and behaviours
CBT interventions typically focus on changing unhelpful thoughts and behaviours to shift the whole system. For example:
Cognitive techniques help you identify and reframe unhelpful thoughts (Maybe they’re just having their own conversations and not thinking about me at all).
Behavioural techniques encourage experimenting with new actions (staying in the room, initiating small talk) to test those thoughts and build new patterns.
As children, we lacked the ability to critically assess whether our interpretations of events were accurate - or whether what adults and popular or family cultures told us was actually true.
Our worldview as children conditions how we see things as adults. By testing out our childhood-conditioned thoughts and behaviours, we can generate evidence against our old beliefs and rules and for more realistic and helpful alternatives.
The strengths and limitations of the Standard CBT Model
The Standard CBT Model is an excellent starting point for understanding our internal experiences. It’s structured, clear, and evidence-based. But - as we’ll explore in the next few articles - it has some limitations for ADHDers and others who experience strong emotional dysregulation, alexithymia, or Rejection Sensitivity Dysphoria.
Why ADHDers need an Enhanced CBT Model
ADHDers often struggle with standard CBT because:
frequent amygdala hijacks override the ability to think rationally. A hyper-activated amygdala initiates a fight-or-flight response, literally switching off the neural circuits to the prefrontal cortex, where logical thinking sits. It becomes almost impossible to challenge your automatic thoughts and emotional reactions when you are overwhelmed and overwrought.
alexithymia is the stable tendency (or trait) to find it difficult to identify and express emotions (there’s no difficulty in feeling emotions, just in labelling them). It affects approximately 10% to 13% of the general population. However, among individuals with ADHD, the prevalence is notably higher, at around 40%. Therefore, ADHDers might need workarounds to help identify emotions before starting out with the standard model.
Rejection Sensitivity Dysphoria (RSD) is an intense emotional response to perceived rejection, criticism, or failure. It is not simply about disliking rejection - it’s a visceral, overwhelming reaction that can feel unbearable, often triggering deep shame, anxiety or sudden anger. Even minor criticisms or neutral interactions can be misinterpreted as signs of disapproval, leading to avoidance, perfectionism, emotional outbursts or withdrawal. RSD is particularly common in ADHD, where heightened emotional reactivity and difficulty with self-regulation amplify the distress. ADHDers with RSD may perceive the work done in CBT as personal criticism. Therapists need to be mindful of this, and clients benefit from having it clearly explained to them.
We will further flesh out these limitations of the standard model of CBT in the next few articles.
Call to action
For now, try reflecting on a recent situation where you experienced a strong unwanted emotion. Complete a standard CBT model of how that problem is being maintained and how it may have developed - download below.
Here are some stepwise prompts:
bring to mind a strong and unwanted emotion that you experienced recently
what was the situation that this emotion occurred in?
at the peak of that emotion, what thoughts or images were in your mind?
what physical sensations accompanied this? What did I notice in my body?
what were your behaviours - What would a camera have seen you doing? What did you do to cope and get through it? What didn’t you do? What did I avoid doing?
See you next time, for my Enhanced CBT Model for ADHDers.

Get more of what you want and less of what you don’t - manage your Substack experience by clicking here.

Thank you so much for this!! I am going to share this with my neurodivergent community- a lot of of us struggle with some aspects of CBT, while other aspects are so incredibly helpful
This explains a lot
Thank you for this. I'm indebted to CBT and ACT for becoming a functional person, who often feels RSD. However, I didn't realize that RSD is particularly common in ADHD. I haven't been diagnosed with ADHD, though I suspect myself to have CPTSD, which I've read has symptoms that overlap with ADHD.